While employed with Caris Lifesciences I rewrote many standard operating procedures (SOP). For many of them I had to start from scratch so that they were legible. A lot of the time text was just copied from the instructional manual that came with instruments. I changed a lot of that and wish I could share them with you.
We were lacking many SOPs for processes, and I created many to fill that void. All of them went through a review process, and all the ones I wrote were widely accepted. Also, I implemented photos into the SOPs so they were much easier to read. The images really help break up the text, and as everyone knows, a picture is worth a thousand words.
When this instrument came into the lab, I was sent to the Tucson location of Ventana Medical Systems for training on this instrument. It’s a completely modular system that is easy to fix by simply replacing the system that is broken. Just like the Benchmark XT, these machines pretty much ran non-stop during the operating hours in the lab. Many people fault this machine because it does break down because of the complicated transportation system it employs, but it’s easily fixed by a Ventana representative by simply replacing modules.
These are the most widely used IHC stainers in histology. These machines were kept operating on a 24hour basis 7 days a week. They only came down for maintenance, repair, and decontamination. I’m really surprised that they didn’t break down more. Ventana reps were always fixing them, but only because they basically operated non-stop since they hit the production floor. Amazing work horse machine that does beautiful staining.
I was also in charge of doing decontaminations on these instruments.
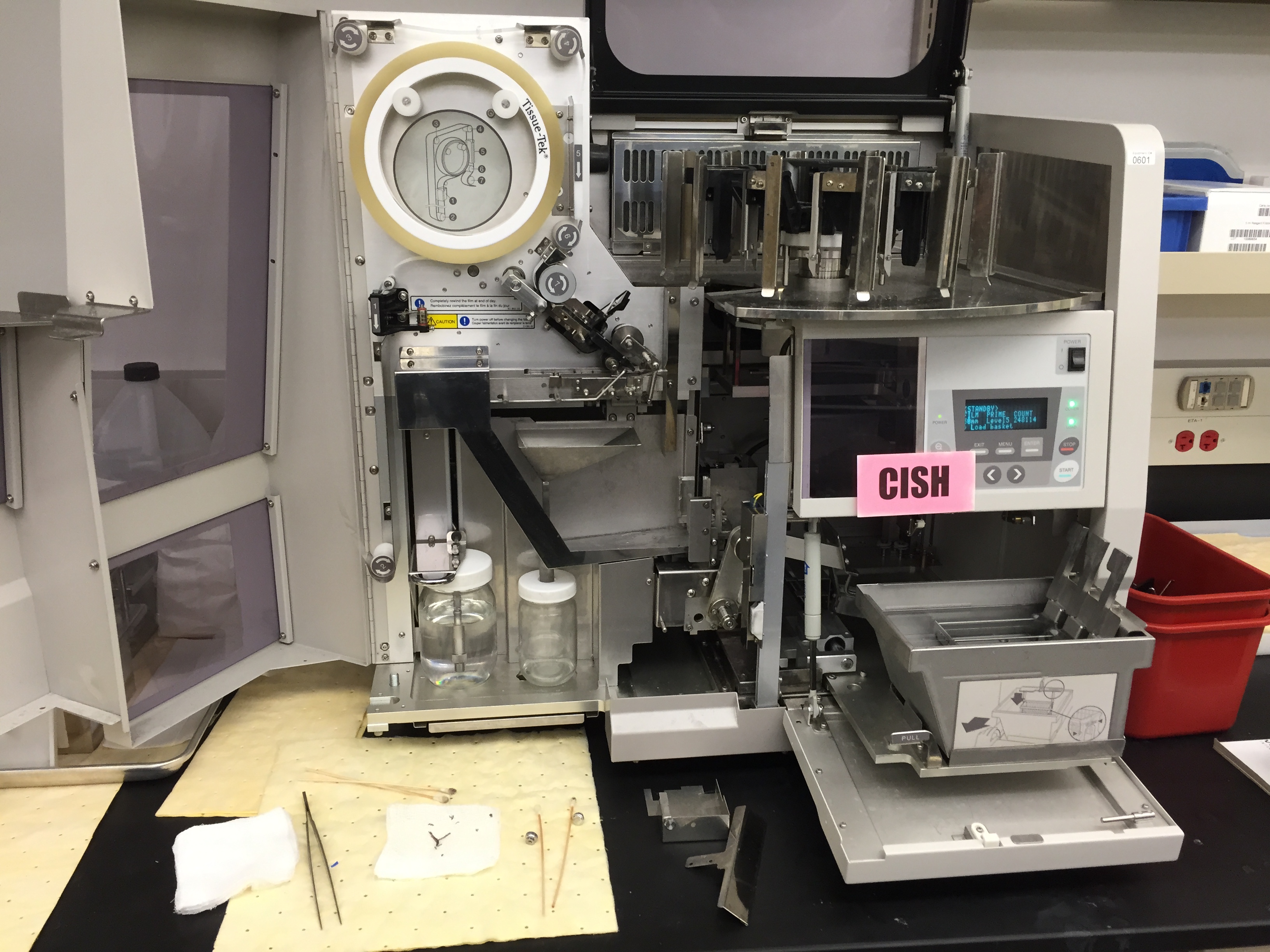
I didn’t a chance to use this system that often. It operated like a benchmark XT, but with more flexibility over what it could stain on each slide. Caris Lifesciences was starting to utilize CISH staining, and this machine was quite often used for that, or repeat IHC slides.
I was in charge of doing the decontaminations on this machine. Ventana made it pretty simple to do.
Sakura Tissue-Tek Prisma Stainer utilizing dip cup staining
This instrument was used for many different applications at Caris Lifesciences. We first used it to stain H&Es, but that was replaced when we got a Ventana Symphony. Then we used it for random stains and things, but finally ended up staining nuclear fast red (NFR) stain in it to preempt microdissection. It’s an easy to use stainer since there are no complicated mechanisms, nozzles, or equipment. There’s an arm that pulls up slides in a basket and dips them in a cup. Maintenance was easy on it as well. Each day the reagents are dumped out and new ones added to the cups. The software was pretty easy to use as well.
The Sakura Tissue-Tek Film Coverslipper was used extensively in the lab. It operated great, once it was cleaned, and coverslipped all of our slides. This machine is a workhorse and I would highly recommend its use. There is only one drawback to the system, the stickers we used to identify each slide, had a xylene soluble adhesive which would soften and gum up a lot of the moving parts the slide touched in this machine. So once a week, or more often depending on workflow, the machine needed to be thoroughly cleaned. Most people did not know how to do this, so it usually came down to me to make it happen.
Once of the drawbacks of the film vs glass coverslipping is longevity. The film remains clear for only so long, whereas the glass ones are indefinite, or until the adhesive drys out. We rarely needed to use glass coverslips, and only then on broken already stained slides.
Aside from the RM2235 manual microtome, I’ve used one of these extensively. I’m not sure that anyone in the histology field actually uses the foot petal to automatically rotate the microtome. When cutting samples you need to be able to feel how the specimen is cutting, which you can not if you aren’t manually operating the rotary mechanism. This instrument does provide very smooth, less noisy, cutting action. I really like using these microtomes. Both the RM2235 and this RM2255 work excellently for cutting the specimens we received at Caris Lifesciences.
Tissue processing is a technique used to desiccate tissue using alcohol. The tissue still needs to have some water in it though, otherwise it would just be as hard as a rock and impossible to cut. There is also the possibility of the tissue receiving incomplete dehydration due to the thickness of the tissue. If it’s too thick, the alcohol can’t penetrate far enough into the tissue. Thankfully, if the gross dissection was done properly, the tissue was just the right size for our validated processes.
This is a Sakura Tissue-Tek tissue processor similar to the one Caris used
We used automated tissue processors at Caris Lifesciences, but they were validated using hundreds of samples to make sure that the process worked well. We had several different run profiles that would work for large samples, medium samples, and small samples. The only thing that changes between the profiles is the length of time that the tissue sits in the alcohol. The alcohol is used to dry the tissue, then it goes through steps of xylene which removes the alcohol from the tissue. Depending on the process, this can happen multiple times, or the xylene can be introduced as the final step before paraffin infiltration. The final step of tissue processing is the introduction of paraffin. The paraffin is usually pressurized to help infiltrate into the tissue. This is usually the longest step and important for successful microtomy.
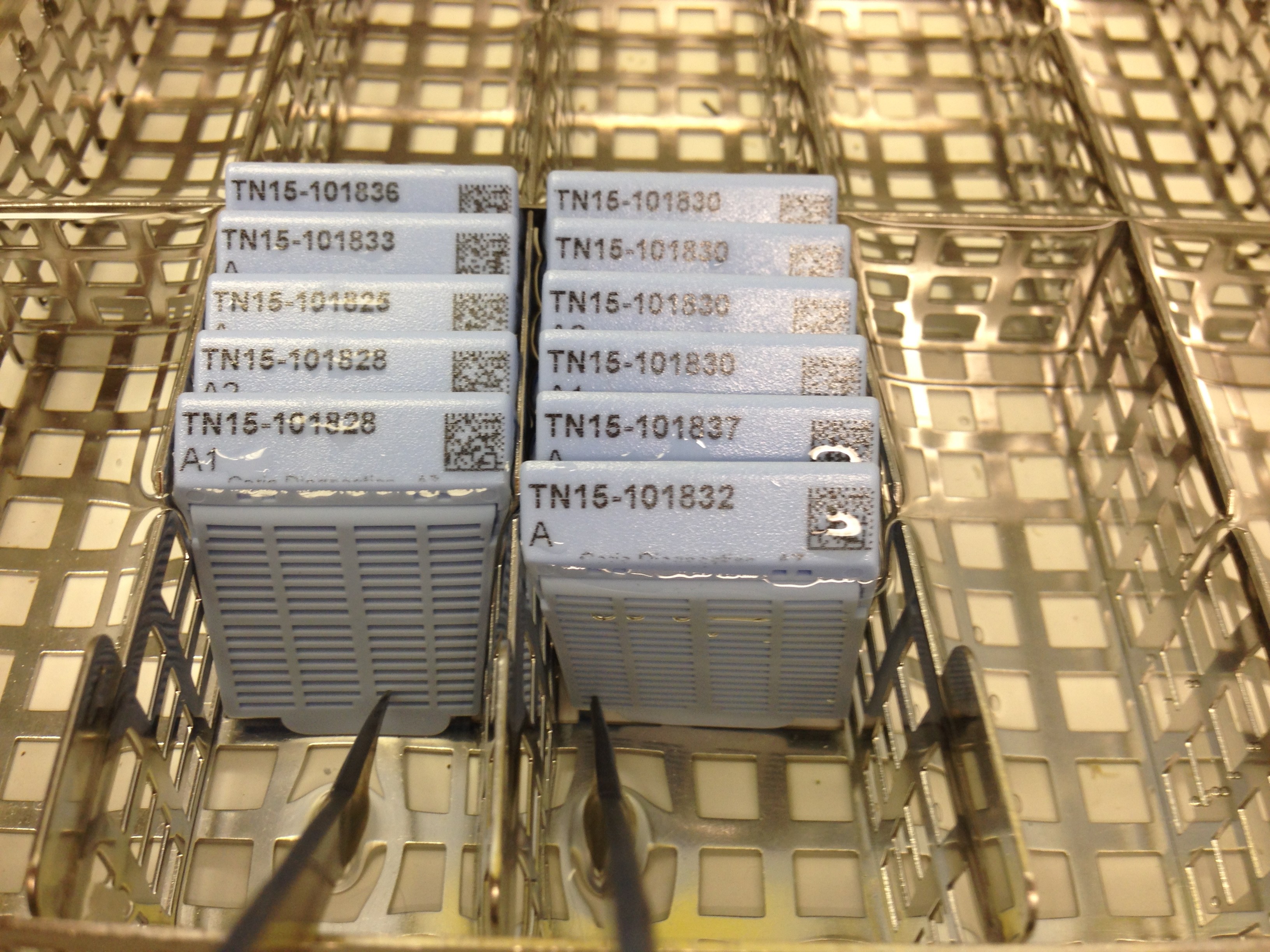
Plastic cassettes used in the tissue processor. On the side facing the photographer, there is a little plastic mesh door that is closed over the tissue so the tissue doesn’t escape during tissue processing
The tissue processing we did required that the tissue already be fixed in formalin. We didn’t have a process for doing fresh tissue, since the company never had to deal with it. There were some times that we were trying to process cytological specimens, and those were difficult to get processed. We would have had to validate a new process for those, but that didn’t happen while I was employed there.
This is easily the most complicated process performed in the immunohistochemistry (IHC) lab at Caris Lifesciences. All of the quality control that is done in the lab is dependent on the TMA. So without these cutting and staining well, the lab comes to a standstill and repeats have to be performed on a large number of tests. This delays production and costs enormous amounts of money. The TMA production was my primary responsibility at Caris. I also developed a method to save the company between 100-350k on bulk tissue costs by implementing a shallower tissue punch in the block.
Awarded after my TMA workflow processes changes were implemented
I can’t go into too fine of detail on the process, but I’m quite familiar with how these are made. I’ve written the complete standard operating procedure (SOP) on this process, and many other processes, for Caris Lifesciences.
The outline of the process for making TMAs is as follows: bulk tissue purchasing, bulk tissue cutting, quality analysis/positive staining, block marking, TMA blank block production, tissue punching, and lastly, quality control.
Bulk Tissue Purchasing
It’s incredibly hard to find a reliable source(s) for tissue and the distribution/purchasing of such tissue is sort of in a legally gray area. The tissue we receive must stain positive, dependent upon tissue type, for the immunohistochemical (IHC) stains we are performing on patient tissue. So this means we need human tissue that has tumor in it. Thankfully the process we have implemented uses the least amount of tissue as possible to maximize the usability of the bulk tissue blocks.
Bulk tissue block
Bulk Tissue Cutting After the bulk tissue blocks are received, each has to be sorted into tissue types and then the tissue types that are going to be punched in to the TMA have to be cut on the microtome. One section for each stain it is suppose to stain positive for must be cut. For some of the tissue types such as HER2 positive breast tissue, only needed one slide cut, but for others, as many as 11 slides per block had to be cut.
Bulk Tissue Quality Analysis Each block has to stain positive for each of the stains it is going to be used as a positive control on. So for each block, the IHC slides must be looked at closely to make sure uniform staining has occurred and it is staining the right sections of tissue. These IHC tests usually stain a certain tissue type the best such as epethilial, nerve, capillary wall, mucousal, etc cells. During the tissue validation phase, all the different tissue types are stained with all of our stains and then a pathologist looks at them to determine which ones they want for positive controls.
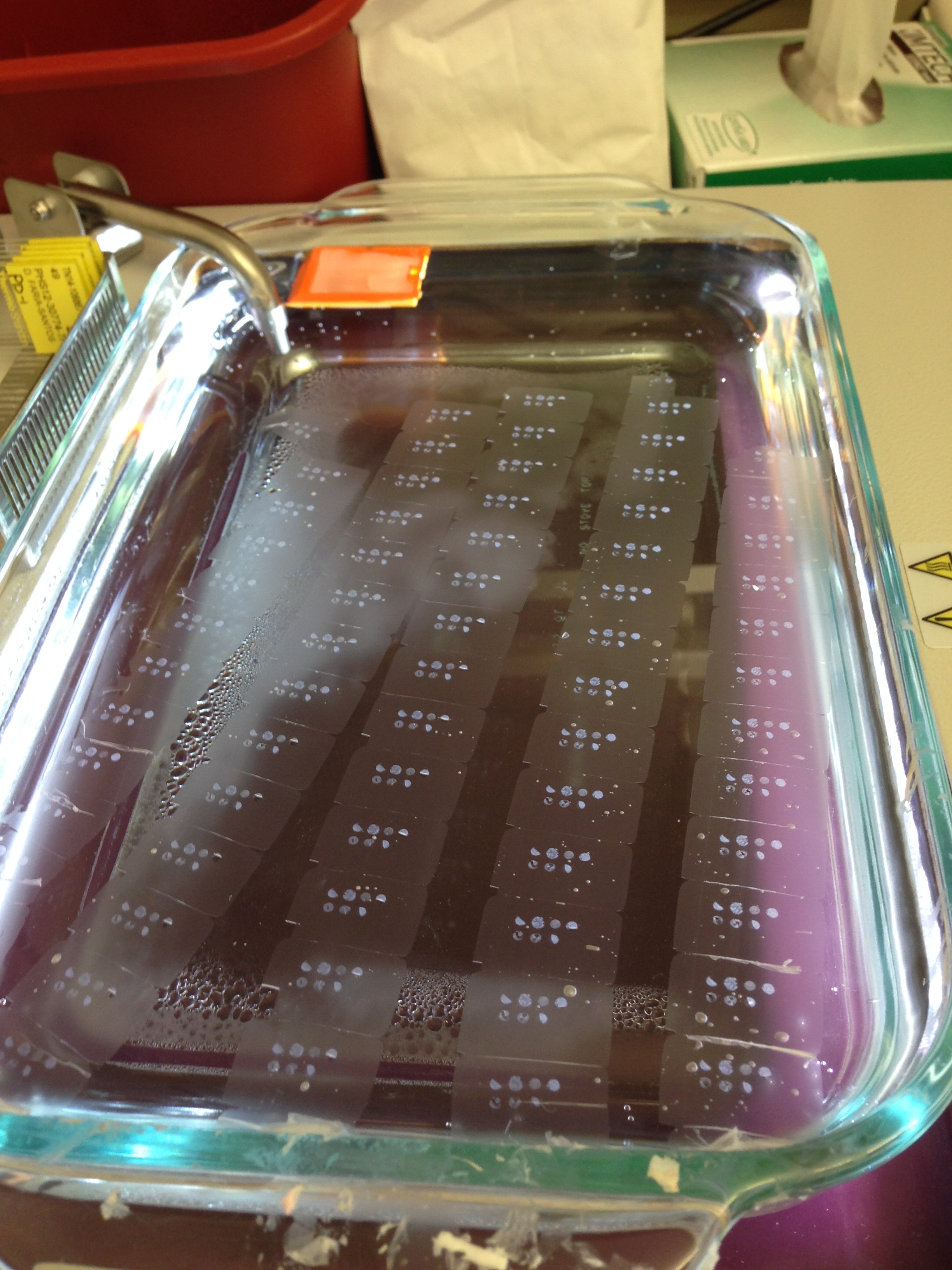
Sections laid out on a warm water bath
As part of the quality analysis of the tissue, once determined that that tissue block is suitable for use in the TMA, the stained slides are then each marked to highlight the area we are interested in punching. These punches go into the blank TMA blocks to make the cutable TMA.
Block Marking
After we’ve determined that the block has stained positive for all of the tests it needs to, the positive portions are marked on the coverslip of the glass slide. These marked slides are then overlaid on the block and used to mark the tissue in the block with a statmark pen.
TMA Blank Block Production Now that there are a lot of blocks marked of each tissue type that is going to go into the TMA, we need to make TMA blank blocks to put the punched tissue into. Depending on the size of the punches and the number of punches for the TMA, a mold size is chosen. Plastic cassettes, generally of a different color than the patient specimen color, are printed out and placed on top of each mold. Paraffin is poured in the mold and then the perfect amount of paraffin needs to remain in the back of the plastic cassette. Without the paraffin backing the cassette, it’s really easy for the portion in the mold to fall off when cutting the cassette or punching through the plastic cassette when making the TMAs.
Tissue Punching
MTA-1 manual tissue arrayer
During this step a predefined set of coordinates is used to punch certain tissue types into certain areas of the block. To streamline the punching process, I would set the instrument to the first coordinate and recipient-punch all the blank TMA blocks at that location. Line those up, usually 10 at a time, and then use the bulk tissue blocks and donor-punch them set aside the cores on a cutting board. To prepare the cores for the blank TMA blocks, the paraffin on the bottom has to be sliced off using a scalpel. The tissue is then stacked in the hole on the donor block (blank TMA block). The whole process then repeats itself for each coordinate.
Quality Control of the Finished TMA Block Once a block has been fully completed, through trial and error, we figured out that baking the blocks for a set amount of time helped embed the tissue cores in the paraffin a little better. Most TMA blocks have problems with the tissue cores being pulled out by the blade during microtomy.
TMA sections laid out on a water bath
Once they are cooled a couple sections are cut off each and they are stained H&E to look for the correct cell morphology in each core, and then put them into production. Each microtomist gets a block and uses it to cut a section on each slide that already contains patient tissue and that is also going to be stained one of the IHC stains we did at Caris.
These are completed and nearly exhausted TMA blocks